1982
Act
Information
Official
the
under
Released
Document 1
Why is Pfizer developing a separate paediatric vaccine?
8.
There are several potential technical reasons why Pfizer has developed a specific paediatric
version, including that the:
a. the existing adult version may not be stable at the dilutions required for paediatric doses;
b. the practicality of administering a lower volume of the same concentration of the existing
adult vaccine; and
c. using a diluted or smal er volume of the adult vaccine would require the vial bung to be
punctured a large number of times. For other medicines we know this increases the risk of
smal parts of the bung entering the solution or introducing bacteria into the solution.
9.
A meeting between our Science and Technical leads and Pfizer’s is being co-ordinated to further
1982
understand Pfizer’s paediatric product.
If the adult version is used in 5 to 11’s, there are a number of potential risks
Act
10.
If the adult version is used off label, there are a number of potential risks included. This is
because:
a. There are no clinical trials to demonstrate safety and efficacy of the whole formulation
(including the content and quantity of other ingredients). This means there would be no
data supporting the safety, efficacy and quality of the existing vaccine vials when used in 5
– 11-year-olds;
Information
b. the vaccine may have degraded before being administered (less viable mRNA leading to
limited to no immune response); and
c. there is a risk of bacterial contamination as noted above.
Official
Timeline for accessing a paediatric product
the
11.
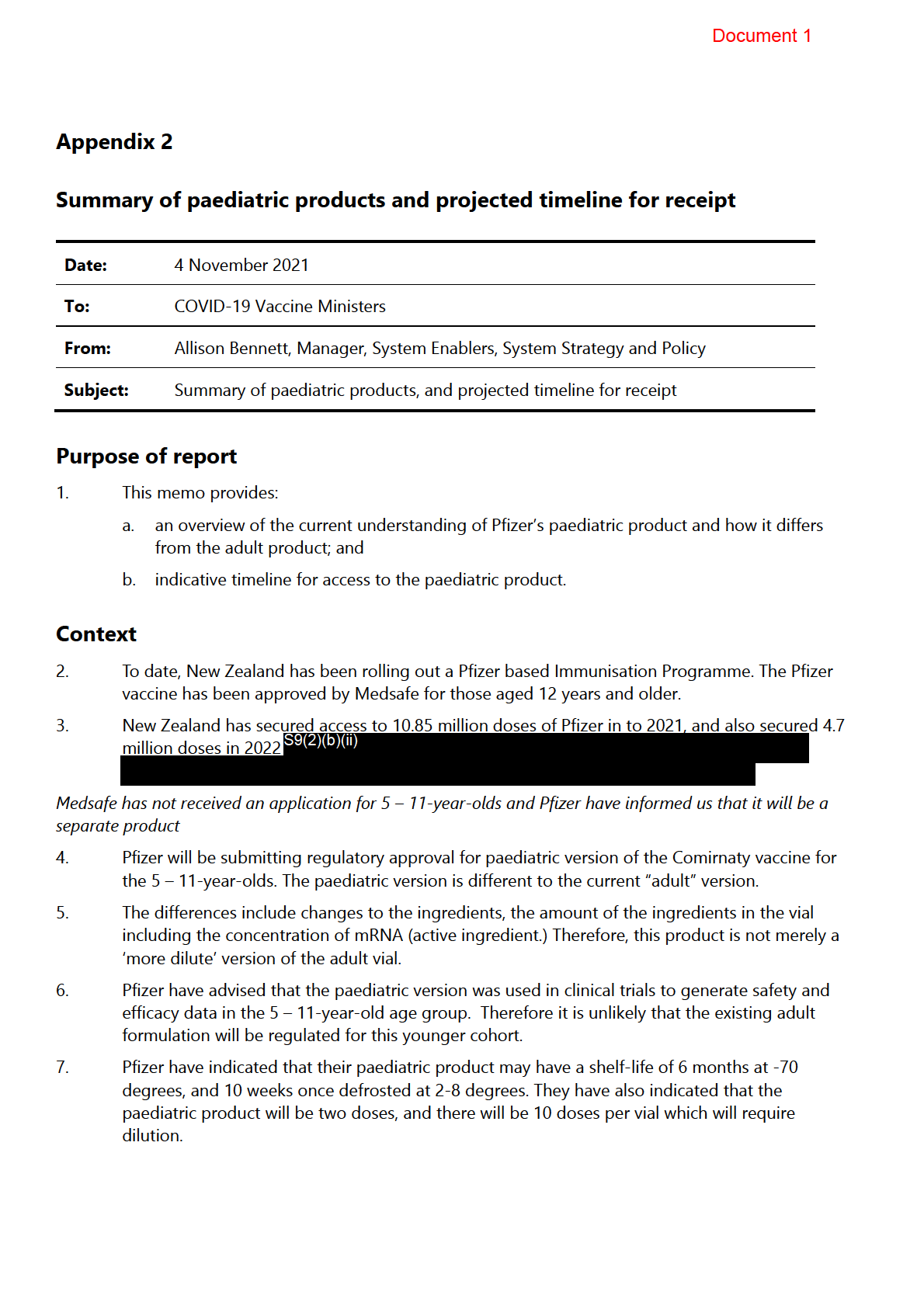
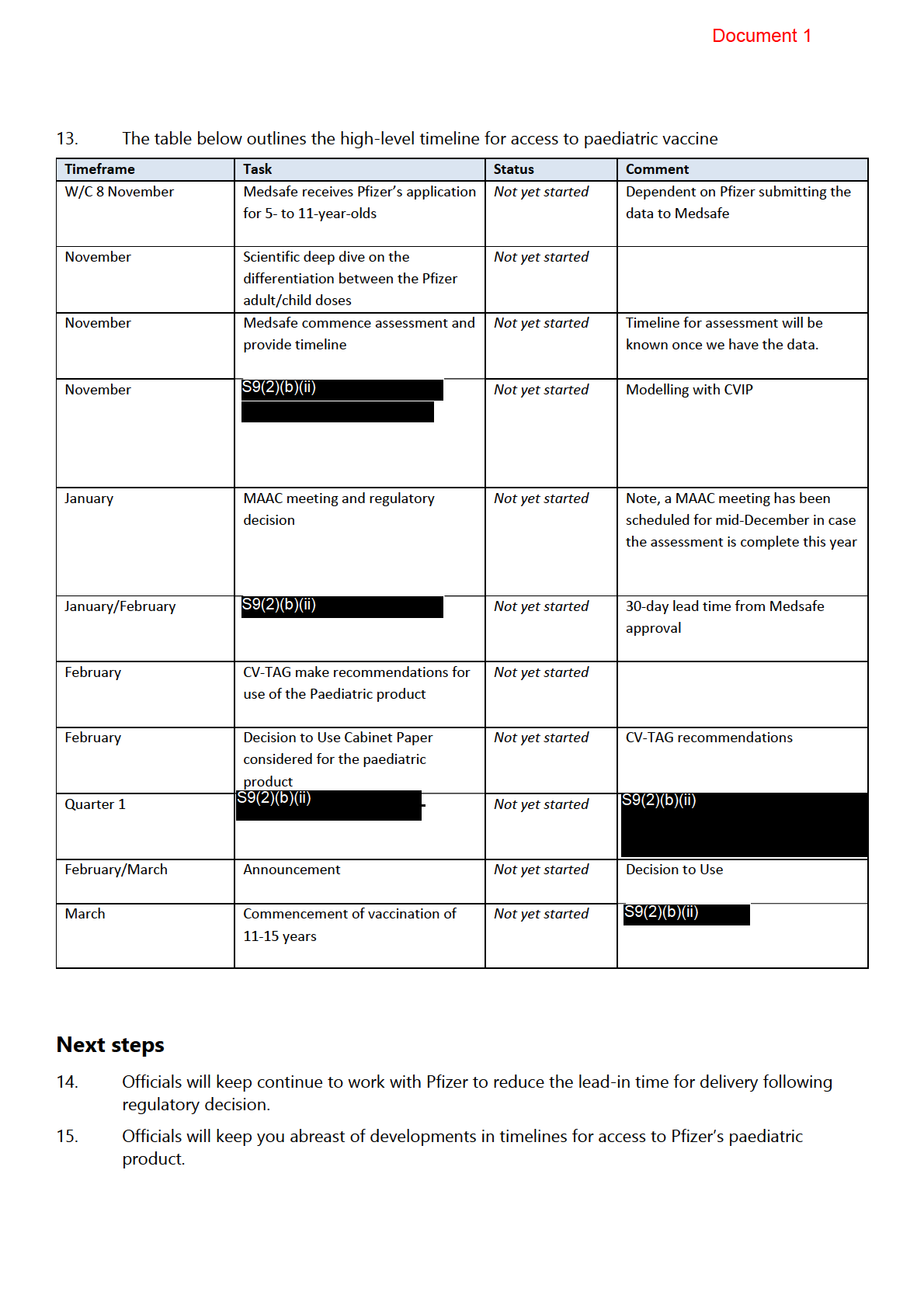
The table below presents a possible timeframe for brining paediatric doses into New Zealand.
Please note, these timeframes are subject to change and are largely dependent on Pfizer.
12.
The key steps to receive doses for 5 to 11’s include:
under
i. Pfizer submitting their application to Medsafe and providing al necessary data
ii. Medsafe’s assessment and regulatory decision
iii. Notification of Medsafe approval to Pfizer to fil the order
iv. the COVID-19 Vaccine Technical Advisory Group assessment and recommendations
Released
v. Decision to Use for this cohort
vi. Receipt of Vaccine
1982
Act
Information
Official
the
under
Released
Document 1
Recommendations
It is recommended that you:
1. note
that Pfizer is developing a separate paediatric product for use in those aged
5 to 11 years
2. note
That Pfizer have not submitted an application for regulatory approval for
their paediatric product to Medsafe
1982
Act
Information
Official
the
under
Released
Document 2
COVID-19 Vaccine and Immunisation Programme
Proposed implementation approach for vaccine rollout for 5–11-year-olds
Date:
26 November 2021
To:
COVID-19 Vaccine Ministers
From:
Jo Gibbs, National Director, COVID-19 Vaccine and Immunisation Programme
Subject:
Proposed implementation approach for vaccine rollout for 5–11-year-olds
1982
Purpose of report
Act
1.
This paper seeks to update you on the high-level approach and implementation plan for the
COVID-19 vaccine rollout for the 5-11 age group in New Zealand, subject to regulatory
approval, CV TAG advice and Cabinet’s decision to use.
Context
2.
The Pfizer COVID-19 vaccine has demonstrated its safety and effectiveness against people
contracting the virus and becoming seriously ill or transmitting the virus
Information to others. Until
recently, the vaccine was not approved by any regulator for use in children under the age of
12.
3.
In September 2021, Pfizer released positive top-line results from their trial of the COVID-19
vaccine in 5-11-year-olds. International regulatory proc
Official ess has since been underway, with the
Food and Drug Administration (FDA) approving the use of Pfizer for this age group in late
October in the United States.
the
4.
Medsafe are currently working through an application to allow the use of the vaccine with the
5-11 age group in New Zealand.
5.
We note that Australia could commence the rollout of vaccines for this age group before the
under
end of 2021 or in early 2022.
6.
To be prepared for rollout as soon as possible, the CVIP programme has commenced
operational planning for this population cohort. Planning for this rollout is taken in
consideration of other current programme priorities:
a. Completing the rollout of two doses to the eligible population of New Zealand, aiming
Released
to achieve 90% percent vaccination across Aotearoa.
b. Ensuring that AstraZeneca is available for those who are eligible.
c. Deploying booster doses for the c. 465,000 people who are eligible before the end of
2021 and ensuring prioritisation for those most at risk.
d. Focus on the equitable, safe and well considered implementation plan for the
vaccination of 5–11-year-olds, that aligns with the regulatory approval, Cabinet
decision, and supply from Pfizer.
Document 2
Implementation
7.
We are undertaking operational planning activities for the 5- to 11-year-old COVID-19 vaccine
rollout with the assumption that Medsafe and CV-TAG advice are expected by mid to late
December 2021. The programme has developed a proposed high-level implementation
approach that will continue to evolve throughout December 2021.
8.
We expect that the rollout will be able to be technically and operationally commenced from as
soon as 17 January 2022. We will aim to secure the product as soon as possible in order to
create certainty of supply as soon as practical.
9.
The time between supply arriving and the beginning of our rollout will allow time for the
workforce training, updates to operating and handling guidelines and to ensure the logistics
are in place. S9(2)(f)(iv)
1982
10. This planning window also allows us to thoughtfully plan our equity approach, create effective
Act
communications for potentially hesitant parents, and to begin the rollout before this age group
returns to school. We will aim to find opportunities to improve this timeline.
11. Our Te Tiriti o Waitangi obligations continue to be an essential element of the planning phase
before the rollout commences. We will leverage lessons learned from the programme to date
and by leveraging our existing partnerships. We are meeting with Pandemic Response Iwi
Chairs next week and will continue to engage them as we develop the rollout and
implementation plan.
Information
12. We are also exploring options for prioritising areas of New Zealand in the first phases of the
rollout. Where practical, we will also endeavour to align this rollout with the booster campaign
(leveraging the whānau-based approach) and other immunisation programmes, such as MMR.
Official
13. Early implementation activities have been undertaken, including preliminary policy work, an
impact assessment of the required technology changes and supply discussions with Pfizer.
the
14. We are working to an assumption that supply could be available S9(2)(b)(ii)
Our logistics and workforce workstreams have confirmed they are able to support the
delivery of the product within this timeframe.
15.
under
Established service delivery models (via Hauora, primary care and community centres) will be
the main sites used to administer doses. They have sufficient capacity to manage the expected
demand of an estimated ~500,0001 5-11-year-olds. Some hospitals, particularly those in
outbreak regions, may choose to provide additional on-site capacity for staff.
16. A high priority for the programme will be to complete the majority of first doses for this cohort
ahead of or as early into the school as possible.
Released
17. A targeted communications campaign will support the delivery of this rollout. An assessment
of specific channels, stakeholders and providers that will reach the parents and guardians of
this population cohort is underway.
18. Strategic communications planning is also underway to prepare for timing announcements,
and likely media reaction as other jurisdictions commence their rollout for this age cohort.
1 Stats NZ 2021 population projection (2018 Census)
Document 2
Risks
19. The programme must plan for equity from the beginning of the planning phase of the
paediatric COVID-19 vaccine rollout.
20. International experience suggests that hesitance could be higher for the paediatric COVID-19
vaccine amongst parents. A careful and thoughtful implementation plan and public
communications plan at the beginning of the rollout will be essential to increasing uptake
throughout the programme.
21. The safety and delivery of the vaccine will be especially important and sensitive for the rollout
to younger age cohorts and must be carefully managed both within the programme and the
public.
22.
1982
It is possible that the delivery timeline of the product is delayed if the Medicines Assessment
Advisory Committee (MAAC) requires additional data from Pfizer before making a decision.
S9(2)(g)(i)
Act
23. Global supply chain or Pfizer supply disruption could delay the time frame for the rollout.
Next steps
24. Officials will continue to work on detailed implementation planning.
25. A further update on this work will be provided by 10 December 2021.
Information
26. A decision to use is expected to be submitted to Cabinet as soon as practical.
Recommendations
Official
It is recommended that you:
the
1 Note
The risks associated with the 5- to 11-year-old rollout planning and timeline.
2. Note
That the Ministry of Health will continue to progress operational planning and
readiness activities
under for the COVID-19 vaccine rollout to 5- to 11-year-olds.
3. Note
The current timeline and high-level implementation approach for COVID-19
vaccinations for 5- to 11-year-olds.
4. Note
That rollout for 5- to 11-year-olds is subject to a Medsafe regulatory decision,
CV-TAG advice, and Cabinet’s decision to use the Pfizer vaccine for 5- to 11-
Released
year-olds.
1982
Act
Information
Official
the
under
Released

1982
Act
Information
Official
the
under
Released
1982
Act
Information
Official
the
under
Released
1982
Act
Information
Official
the
under
Released
Document 4
Appendix 8
1982
Act
Information
Official
the
under
Released
Document 4
1982
Act
Information
Official
the
under
Released
1982
Act
Information
Official
the
under
Released
1982
Act
Information
Official
the
under
Released
1982
Act
Information
Official
the
under
Released
Document 4
Ml:--1\1 R) ()f
HEALTH
MAt,.Alf. HAl'OkA
Next steps
28.
The Ministry is preparing advice for delegated Ministers to support decisions on whether to
use the Pfizer paediatric vaccine for children aged 5-11 years in New Zealand.
29.
That advice will include further details on the advice from Medsafe and CV TAG as well as more
details on the planning for the roll out of delivery of COVID-19 vaccines for children in this age
group.
30.
Cabinet is considering its delegations for these decisions this week.
�
Signature
/" f
_5
Date: IS:-/ P/2.\ 1982
Act
Maree Roberts
Deputy Director-General, System Strategy and Policy
Information
Official
the
under
Released
Page 6 of 6
Document 5
National Immunisation Programme
UPDATE: 5 – 11-year-old vaccination rollout
Date:
13 January 2022
To:
COVID-19 Vaccine Ministers
From:
National Immunisation Programme,
Subject:
5 – 11-year-old vaccination rol out
Background
On 20 December 2021, Cabinet agreed to use the Pfizer COVID-19 paediatric vaccine for children
1982
aged 5-11 years with a rol out planned to start from 17 January 2022 (CAB-21-MIN-0557 refers). On
this date, approximately 477,000 children between the ages of 5 and 11 will become eligible to get
their first dose, with a second dose to be administered eight weeks later.
Act
As part of this decision, officials committed to reporting back to the group of Ministers with the power
to act over the holiday period on the implementation approach prior to opening up invitations for
children aged 5-11 years. This report back was to reflect the lessons learned in the initial phase of the
vaccination programme and include an update on the ongoing co-design process currently underway
with hauora providers and iwi representatives.
Information
Approach
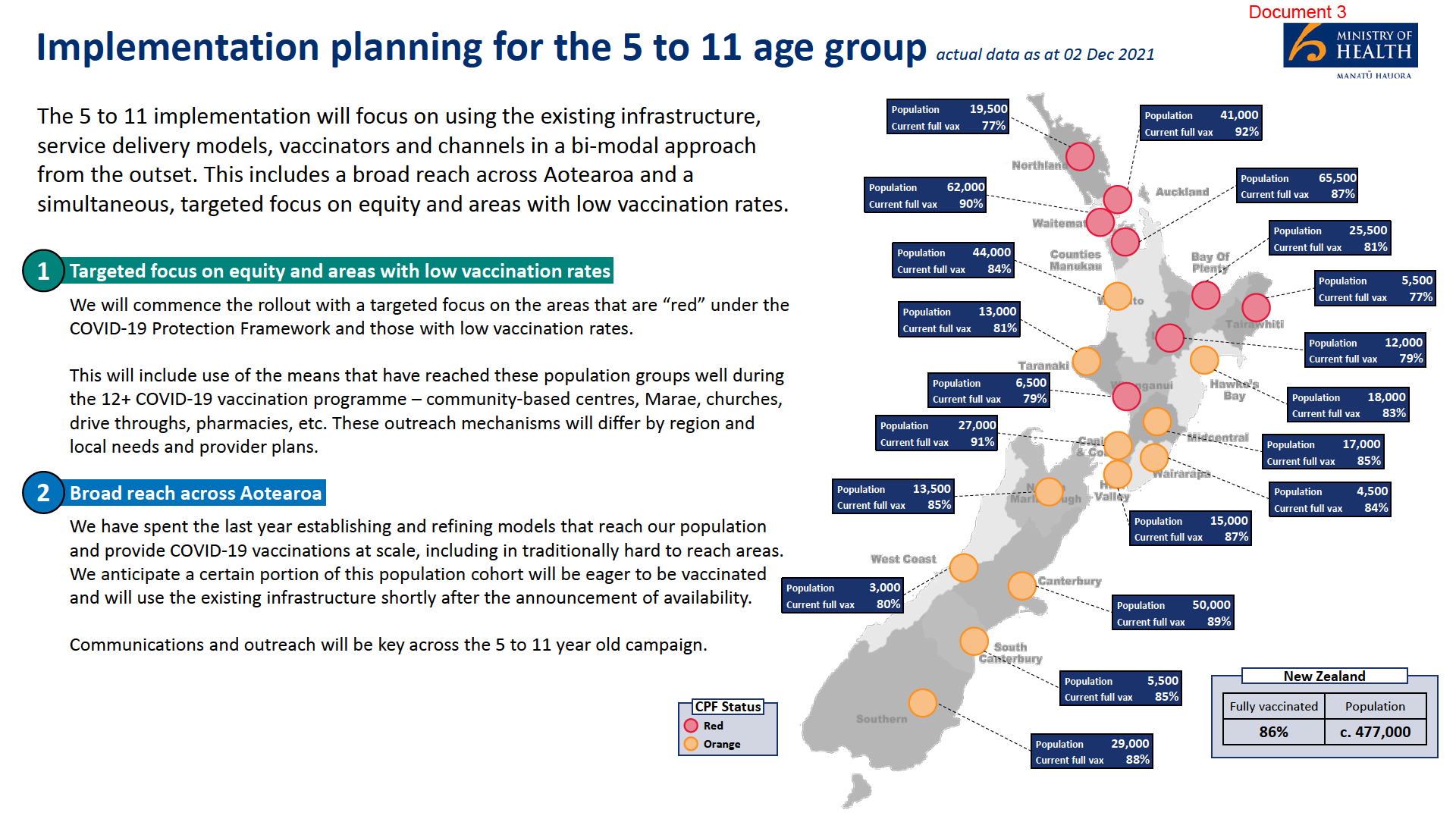
Rol ing out the vaccine to 5–11-year-olds wil make use of the vaccination infrastructure – delivery
models, workforce, technology and logistics – that has been built over the COVID-19 vaccine
programme to date. This wil enable both a broad reach across Aotearoa and a simultaneous, targeted
Official
focus on our priority populations and can be achieved due to the capacity that has been built
throughout 2021 and sufficient supplies of the paediatric vaccine, now in the country, to provide a
first dose all eligible children.
the
International experience shows that childhood COVID-19 vaccination campaigns are different from
those of older children and adults. For example, hesitancy amongst parents is higher, and
under
communications for caretakers and children must be different. Also different to the rol -out of COVID-
19 vaccination to adults, children aged 5-11 wil not receive individual invitations to receive a vaccine.
The emphasis wil instead be on communications for whānau and communities, advising of the
benefits and availability of the vaccine for 5–11-year-olds. A whanau-based approach wil be
strengthened by providing opportunities for families to be vaccinated together, bringing together the
5-11 rol -out, COVID-19 boosters and other scheduled vaccinations wherever possible.
Released
Through the rol -out of the vaccine to the general population in 2021, the system has learnt to keep
monitoring the delivery of COVID-19 vaccinations and adjust the approach where needed based on
feedback and results. The rol -out to 5-11s wil be the same. For example, 5-11 vaccinations will
commence before the start of the school year, but the Ministry and partner agencies wil keep
under review the role schools and school sites might have in maximising uptake of the
vaccine.
The initial roll-out of the COVID-19 vaccine also highlighted the importance of local providers and
trusted community leaders leading vaccination efforts and adequate resourcing for these efforts. To
Document 5
date, funding has been assigned for specific communications for the 5-11 rol -out, but no other
resources have been identified as required above and beyond what is already available for the COVID-
19 vaccination programme more broadly.
A cross-agency approach has also been proven to be effective in supporting the vaccination effort and
the wider community needs associated with responding to COVID-19. The Ministry is working across
government, including with the Ministry of Education and Oranga Tamariki on approaches to reach
children.
Communications
We are taking a three-stage approach to the introduction of the child (paediatric) Pfizer vaccine for
COVID-19, based on research and insights, including on-the-ground insights from providers and
communities.
1. Inform and prepare
1982
• The first phase (current) runs for a month over the summer, across press, radio, social and
digital, including community newspapers and ethnic radio stations. Media activity has included
Act
the announcements of the Medsafe approval and Cabinet decision to use.
• Its purpose is to provide positive, high quality information for parents and caregivers on the
importance of having their tamariki immunised in 2022 without being overly persuasive or
applying pressure.
• The leading voices are paediatricians, particularly Māori and Pacific, and we have worked
closely with the Iwi Comms Collective (ICC) and Maori communications specialists from the
Information
three Auckland district health boards (via the NRHCC) on the advertising campaign. In
particular, two ICC members and two members of the NRHCC have worked alongside CVIP on
the campaign with our agency (Clemenger BBDO) to ensure a Māori communications
perspective is included from the start. Official
• The work is also informed by a group of communications specialists who meet regularly –
members are from NIP (including our disability comms specialist), the NRHCC, Ministry of
the
Education, Te Puni Kōkiri, Ministry of Pacific Peoples, Te Hiringa Hauora (Health Promotion
Agency) and the ICC.
2. Engage and vaccinate
under
• The second phase starts on January 17 when vaccinations for 5–11-year-olds begin.
• Its purpose is to encourage parents/caregivers to book an appointment for their children
(or walk up at sites offering walk-ins or drive-throughs) and to take other whānau
members who need boosters or their first or second doses.
Released
• Vaccination sites wil have products for children (including stickers and activity packs) and
take-home information for parents/caregivers to support a good vaccination experience.
Phase 2 overview:
• January 17 wil begin with a PR (issued Sunday and embargoed) and morning media round
featuring one or more of our key paediatricians.
• The Book My Vaccine website wil be updated with prominent information on the home
page and there wil be updated information on the MOH and UaC websites. DHBs and
providers wil also update their websites and other information.
Document 5
• Radio (attached) wil run across al networks – including Iwi stations and other ethnic stations
with translations.
• TV (storyboard visuals attached) wil begin on the 17th, and social and digital advertising will
change its message to talk about getting your children vaccinated ‘now’ (storyboard visuals
attached).
• Our brochure wil be distributed through places parents and children visit regularly,
including GPs and Hauora providers, schools and kura, councils, and agencies such as MSD
and Kainga Ora.
• Later in January (dates to be confirmed) we wil hold a Facebook Live Q&A session hosted by
S9(2)(a)
and wil do a nationwide household letterbox drop with a combined
message on getting your whānau protected against COVID-19, particularly Omicron –
promoting boosters, child vaccinations, and general y encouraging people to make sure
everyone in their whānau is up to date with their vaccinations.
1982
3. Target and motivate
Act
• From early February, communications activity wil evolve to make the case for paediatric
vaccination to different groups of parents/caregivers – based on new consumer research (in
the field in late January), stakeholder insights and vaccination data.
• The purpose of this phase is to strongly motivate parents/caregivers and address any
barriers to deciding to vaccinate their children.
• Influencers and community champions, including parents/caregivers wil feature alongside
Information
clinicians and we will use specific strategies to respond to misinformation, guided by
research and insights.
Pacific communities
The implementation approach for vaccination of Pacific chil
Official dren wil build on the success of the equity
response and the lessons learned from the vaccination approach for Pacific adults. Primarily this
approach was premised on high engagement, community ownership and leadership and ethnic
the
specific communications. To this end, the first Pacific health sector zoom fono was led by Minister Sio
in December 2021. The fono provided Pacific health providers and leaders with the indicative
timeframes for the rol out of the vaccination for children. This week another national zoom fono led
by Ministry for Pacific peoples and Moa
under na Research with Kids First Paediatric specialist, Dr Teuila
Percival and supported by Director Pacific Health, Gerardine Clifford-Lidstone is being held.
The Pacific Health team have boosted the Prepare Pacific Community Vaccination Fund with a further
investment of $1m to support Pacific child vaccinations. The purpose of this fund is to directly
support Pacific community-led initiatives towards increasing vaccinations. The Fund is commissioned
by the Ministry and administered by The Cause Col ective in Auckland. The fund enables communities
Released
to develop and define their own approaches to improving vaccination rates within specific
cohorts. The additional investment is specifically for improving vaccination rates with Pacific 5–11-
year-olds.
Communications plays a very important role in mobilising the Pacific community. Working with the
NRHCC Pacific team, a further investment of $1m has been made to provide ethnic specific
communications and social media for the Pacific community for booster shots and child
vaccinations. While this investment wil focus on the northern region where two-thirds of the Pacific
population reside, a lot of the information wil be shared across the country on various ethnic specific
Document 5
communication platforms. A smal er al ocation of funding has also been provided to CCDHB and
HVDHB, regions which also have a higher proportion of Pacific communities.
The Ministry for Pacific Peoples has commenced translation of information for Pacific communities
and has developed a specific work programme to support Pacific child vaccinations.
Vaccinating Tamariki Māori
The approach to vaccinating tamariki Māori builds on the learning that more engagement and co-
design in the early stages is likely to achieve a more successful vaccination campaign. To date in
planning for the rol -out to 5-11s, there has been wananga and feedback received from: Iwi chairs;
Māori teachers and principals; Māori pandemic response group, NZ Māori council; and Hauora
providers. Over the holiday period, data was compiled (including risk maps, vaccination data, co-
morbidity stats, school data) and discussed with the Māori pandemic response group to enable better
targeting of efforts in regions.
The fol owing key principles have emerged from engagement to guide the 5-11 rol -out program
1982me,
with a particular emphasis on an events-based approach:
Act
• Whānau orientated - the programme wil be inclusive of the entire whānau and employ a festival
atmosphere that includes Kai, music fun activities, back to Kura Kits and health checks and
vaccination.
• Back to school initiatives and support – back to school preparation and packs are encouraged.
• Data driven - this programme wil be data driven with data being shared with iwi. A separate
Māori data group has been formed with data being shared and col aboration on plans and target
Information
areas.
• Communications - The Iwi Communications Collective, Iwi and agency communications teams will
work together to design and implement a communications campaign that wil be enable local
communications by providing tautoko from national teams. We will also look to kick off the
Official
programme in regions with a strong communications network to ensure information is being
provided to whānau.
the
A range of events have been organised to begin from 17 January, with an increase in events and
activities during February. These include events arranged after school and on weekends that are
celebration focussed and include the whānau. A detailed update about events and percentage of the
under
population targeted with these events wil be provided in the coming weeks. A specific event with
Minister Henare is being planned for late January.
Vaccinating disabled children
To date through the delivery of the COVID-19 vaccination programme, significant efforts have been
made to ensure vaccination sites are accessible for disabled people. This work provides a good basis
Released
for supporting the vaccination of children with disabilities.
DHB readiness
The Ministry has been working with DHBs to prepare for the rol -out to 5-11s. An operating policy for
5–11-year-old vaccinations and operating guidelines were uploaded to the Ministry’s website for
DHBs to access prior to Christmas. Using this guidance, each DHB wil be providing assurance on their
operational and clinical readiness to start vaccinating this age group by 17 January.
DHBs have also been asked to provide an implementation plan for the COVID-19 vaccine rol out to 5-
11s to the Ministry by 17 January. This wil provide a broader picture of each DHB’s planned approach
Document 5
to extending the existing vaccination delivery system to reach 5–11-year-olds with a particular focus
on priority populations.
Vaccination sites and vaccine supply
504,000 doses of paediatric Pfizer COVID-19 vaccine arrived in New Zealand on 8 January 2021 as
planned. S9(2)(b)(ii)
DHBs were asked in mid-December 2021 to identify the sites that would initial y administer paediatric
doses from 17 January 2022. This was to al ow sites to be able to order paediatric doses and be made
available on Book My Vaccine for paediatric appointments. DHBs were asked in particular to consider
the location and nature of providers to support achieving equitable outcomes, focus on areas with low
vaccination rates and promote access.
Some sites are expected to be available to walk-ins from 17 January, but there wil also be sites that
wil be bookable on Book My Vaccine from 17 January. Sites initial y available wil be those already
delivering COVID-19 vaccinations to adults. Other sites such as schools will likely be added as the
1982 roll-
out progresses.
Act
Distribution of the paediatric vaccine to DHBs began on 11 January.
Workforce training
The training module for 5-11s was made available on the IMAC website on 23 December 2021. This
al ows the existing vaccinator workforce (excluding the COVID Vaccinators working under supervision)
to complete the appropriate training on-line. The focus for COVID-19 Vaccinators Working Under
Supervision wil remain for now on vaccinating adults, including delivering COVID-19 vaccine
Information
boosters.
Next steps: Testing of systems and processes prior to 17 January (wet runs)
Between 13 and 16 January, two trial runs of systems and processes wil be undertaken before
Official
vaccinations are open to al eligible children on 17 January:
• The children of border workers in Auckland
the wil be vaccinated between 13 and 16 January. This
trial of systems and processes is being run in conjunction with MBIE and the Auckland metro
DHBs.
• Children in Te Kuiti wil be vaccinated on 15 and 16 January in a test of systems and processes run
under
by Waikato DHB and a local GP.
The findings from these test runs wil be shared with DHBs as part of ongoing learning and process
improvement.
Released
1982
Act
Information
Official
the
under
Released
Document 6
Overview
Childhood immunisation programmes are an essential part of protecting children in New
Zealand and around the world from a range of preventable diseases. These include diseases
that have high mortality (tetanus, meningococcal), high transmissibility (measles and
chickenpox), long term effects (hepatitis B, polio and HPV), or are particularly dangerous for
very young children (whooping cough and rotavirus).
From time to time, new vaccines are developed, adding to the tools available to protect our
health. Normally, these address endemic diseases that we have considerable experience with
1982
and depth of understanding about. The COVID-19 pandemic means we have had to make
rapid decisions about how to deploy vaccines as they became available.
Act
The impacts of COVID-19 immunisation on child wellbeing for children 5 to 11 years old was
assessed to inform decisions on whether and how to use the COVID-19 paediatric vaccine for
this age group. These decisions, and the impacts noted in this report, are subject to Medsafe
approval of the vaccine and advice from the COVID-19 Vaccine Technical Advisory Group
(CV-TAG) to assure safety, quality, and effectiveness of the vaccine.
Key points
Information
Immunisation of the population protects children and promotes their wellbeing
• COVID-19 has had, and will continue to have, significant impacts on children’s health,
development, relationships, and lives. Both COV
Official ID-19 disease and measures taken to
mitigate the impacts of COVID-19 disease significantly impact children’s lives and
development.
the
• Immunisation of Aotearoa’s population against COVID-19 is the single biggest
protection against the disease’s impacts on children’s lives and development.
under
Immunisation of children adds protection and promotes children’s
development
• With or without high levels of population immunisation, immunisation of children
(subject to Medsafe approval and CV-TAG advice to assure safety, quality, and
effectiveness) adds individual protection against impacts on children’s lives and
Released
promotes their development. These protections are especially significant for children
at high risk of severe outcomes, including tamariki Māori, Pacific children, disabled
children and children with health conditions, children living in poverty, and children in
the care of Oranga Tamariki.
Immunisation of tamariki Māori requires concerted focus
• To date, Māori have suffered high impacts of COVID-19 and remain at high risk,
given both multiple risk factors for severe COVID-19 illness, and the very young
Document 6
population structure with 10% of Māori being aged under 5 years and ineligible for
the paediatric vaccine.
• Immunisation of tamariki Māori requires strong focus given their greater risks from
and impacts of COVID-19.
• Immunisation of tamariki Māori through whānau-centred delivery that is designed to
be culturally competent for iwi, hapū, and Māori in a variety of settings can promote
the immunisation of Māori tamariki and whānau, and should be given urgent
resourcing.
Immunisation of children should be supported, but not subject to associated
restrictions for any children
1982
• Promotion of children’s development through immunisation is optimised where
immunisation of children is supported and accessible, parents and guardians are
Act
active participants in the decision for their children to be immunised, and children
themselves are informed about immunisation in a way that is appropriate for their
age and development.
• Promotion of children’s development by immunisation would potentially be
undermined and worsened overall by any restrictions, mandates, certification, record
keeping requirements, or other measures that single out children based on whether
Information
or not they are immunised.
Immunisation of children should promote whānau wellbeing
Promotion of children’s development through immunisation would be enhanced by
Official
delivering immunisation in whānau-centred ways that offer a wide range of health and social
development opportunities and services, without undue delay. Examples include whānau
the
health checks, simultaneous immunisation of whānau members, and providing of a range of
supports to meet whānau needs and aspirations (e.g., nutrition, housing, social, financial, and
legal assistance).
under
Released
Document 6
Contents
Child Wellbeing......................................................................................................................................................... 1
Impact Assessment .................................................................................................................................................. 1
COVID-19 immunisation for children 5 to 11 years .................................................................................... 1
DRAFT 15 December 2021 .......................................................................................................................... 1
Child Wellbeing......................................................................................................................................................... 1
1982
Impact Assessment .................................................................................................................................................. 1
COVID-19 immunisation for children 5 to 11 years .................................................................................... 1
Act
DRAFT 15 December 2021 .......................................................................................................................... 1
Child Wellbeing......................................................................................................................................................... 1
Impact Assessment .................................................................................................................................................. 1
COVID-19 immunisation for children 5 to 11 years .................................................................................... 1
DRAFT 15 December 2021 .......................................................................................................................... 1
Information
Child Wellbeing......................................................................................................................................................... 1
Impact Assessment .................................................................................................................................................. 1
COVID-19 immunisation for children 5 to 11 years .................................................................................... 1
Official
DRAFT 15 December 2021 .......................................................................................................................... 1
Overview ................................................................................................................................................................. 2
the
Key points .......................................................................................................................................................... 2
Contents .................................................................................................................................................................. 4
under
Section A: Proposal details ............................................................................................................................. 6
Summary ............................................................................................................................................................ 6
Context ................................................................................................................................................................ 6
Advancing children’s rights and meeting Children’s Convention principles ............................ 8
Section B: Data, evidence, and stakeholder views ............................................................................... 10
Released
Evidence of proposal impacts ................................................................................................................. 10
Direct impacts for children of COVID-19 ............................................................................................ 10
Direct impacts for children who are immunised .............................................................................. 13
Indirect impacts for all children of some children being immunised ...................................... 14
Indirect impacts for whānau and communities of children being immunised ..................... 15
Significant impacts on children and young people ........................................................................ 15
Document 6
Impacts on different groups of children and young people ....................................................... 16
Implications for Tamariki Māori.............................................................................................................. 20
National Distribution of 5 to 11 Age Group ...................................................................................... 21
Views of Children ......................................................................................................................................... 23
Other stakeholder views ............................................................................................................................ 24
Section C: Summary of Impacts .................................................................................................................. 28
Conclusion of impacts on policy proposal ......................................................................................... 28
Recommendations ....................................................................................................................................... 29
1982
Act
Information
Official
the
under
Released
Document 6
Section A: Proposal details
Summary
This impact analysis examines impacts on child wellbeing of offering COVID-19 immunisation
with the approved paediatric vaccine product to children aged 5 to11 years:
• subject to Medsafe conditions, COVID-19 Vaccine Technical Advisory Group (CV-TAG)
advice and a decision to use
•
1982
with provision through a range of child- and whānau-centred providers and settings
to promote uptake among all children and their whānau
Act
• with special attention to promoting uptake for children at higher risk and children in
communities at higher risk from COVID-19, particularly tamariki Māori, Pacific
children, children in poverty, and disabled children and long-term illnesses
• while upholding rights and wellbeing of all children including those who are not
immunised.
Context
Information
The chief context of this proposal is the COVID-19 pandemic in New Zealand, and its impacts
on children, their whānau, and communities. Additional context includes other childhood
vaccines available on New Zealand’s National Immunisation Schedule.
Official
Pandemic impacts
the
The COVID-19 pandemic and efforts to manage it have had significant impacts for New
Zealand children to date. Impacts for New Zealand children have been considerably lower
than for children in many other countries because of the elimination approach taken up until
under
widespread immunisation could be achieved. However, these impacts may increase as the
Delta variant (among others) continues to spread in communities.
Impacts cross all wellbeing domains, including family, social and peer relationships, learning
and development, economic and poverty-related, health (including mental health, impacts of
family violence, and deferred healthcare), and human, cultural and recreational participation.
Released
Negative impacts for children have been greatest for those living in poverty or situations of
high family stress. Māori and Pacific children have been disproportionately impacted by
COVID-19 illness among community members, and the social and economic consequences
of the pandemic have exacerbated pre-existing inequities for these communities.
This differential impact is expected to continue or increase as these communities are at
relatively higher risk from COVID-19 because of lower vaccination rates (especially among
Document 6
young adults and older children), higher rates of underlying health conditions and
disabilities, and of high-contact living conditions.
Pandemic mitigation and role of immunisation
Immunisation represents the most effective protection available against COVID-19, other
than very restrictive measures such as isolation. Other protective measures such as mask-
wearing and social distancing have significant impacts on children’s activities, peer
relationships, and opportunities for social development.
Broader social, ethical and legal issues around immunisation
Because COVID-19 immunisation is the main protection from disease circulating in the
community, both for individuals and for the wider community, including children and people
1982
at high risk, it has been mandated for people working in certain at risk or public-facing roles
(including for school teachers). It has become a divisive topic in some quarters and the
Act
source of some conflict.
Issues to be examined include:
• the ethics (benefit to children versus benefit to general public) – children aged 5 to
11 years make up some 14% of the NZ population and their immunisation would add
to total coverage for the population and potentially impact the rates of transmission
Information
– in analysing whether to offer immunisation to this population, it is crucial to know
what the risks and benefits are
• producing information designed for children as well as for parents, including disabled
households.
Official
• consent – mandatory vaccination is appropriate in far-fewer contexts for children
than for adults; mandates are unlikely to change behaviour of this age group, who
the
are unlikely to be making own decisions around vaccination. Significant proportions
of caregivers of 5 to 11 year olds have expressed hesitancy or intention to not
vaccinate their 5 to 11 year old.1 Consent/refusal to consent from guardians should
under
not raise consequences for children such as potential exclusion of unvaccinated
children from developmentally important activities (school, sports, clubs, parties etc)
that is not in accordance with the evidence of risk (though it may align with adult
messaging), and risk of increasing equity gaps for children given we know that these
gaps are disproportionately harmful for children compared with adults
Released
• careful consideration of the access to information about vaccine status of a child and
how that information might be used. Unvaccinated children could be at heightened
risk of exclusion informally or formally (in education settings) and of bullying
1 https://www.health.govt.nz/system/files/documents/pages/horizon-research-covid-19-vaccine-
survey-october-2021-1dec2021.pdf
Document 6
• anxiety about COVID and about the nature of the vaccination debate being played
out in public and how to support children deal with anxiety and stress
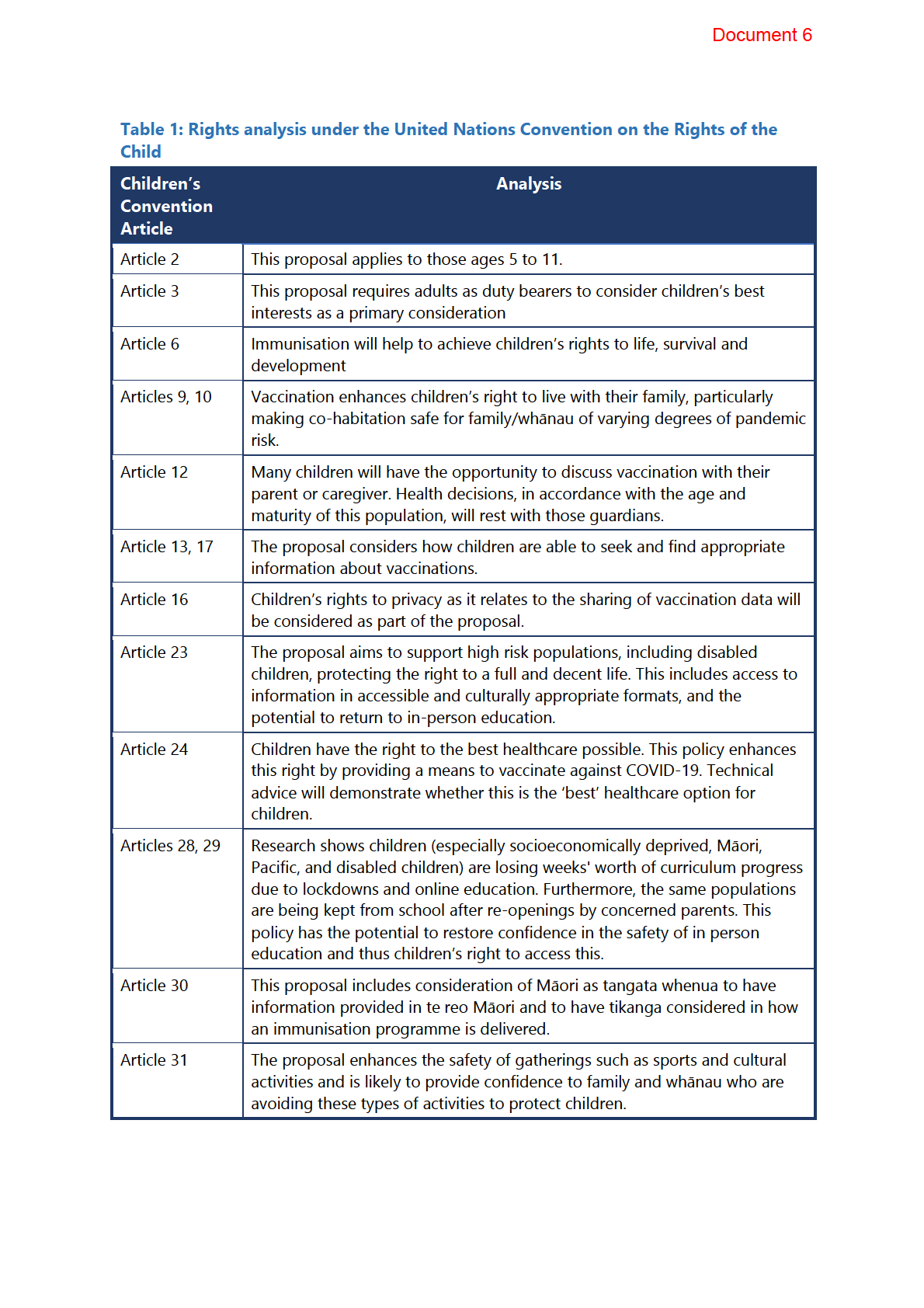
Advancing children’s rights and meeting Children’s
Convention principles
Children live, learn, and grow, not in isolation but as part of families, whānau, hapū, iwi, and
communities. Children have the same basic human rights as adults, but they also have
additional rights in recognition of their special need for protection. Children – particularly
younger children – are dependent on adults, like parents and teachers, to support them to
develop and thrive. These rights are established in the United Nations Convention on the
Rights of the Child. New Zealand has ratified these rights, and they apply to all persons
1982
under the age of 18 no matter their sex, sexual orientation, culture, religion, wealth,
language, or disability status. Below is an analysis of the relevant rights in the convention
Act
and the implication of the proposed immunisation programme on these.
The proposed immunisation of 5–11-year-olds does appear to enhance the rights of
children. The Pfizer paediatric COVID-19 vaccine has a favourable safety profile with similar
side effects to those observed in the 16-25-year-old population.
However, there should not be unintended consequences for children in terms of
Information
participation in in events or access to locations based on vaccination status, as this risks
exclusion and an inability to fully participate in activities crucial for development such as
schooling and extracurricular activities. Such exclusions would likely impact communities
already experiencing disadvantages and where current vaccination rates are poor, potentially
Official
breaching Te Tiriti o Waitangi principles of equity and tino rangatiratanga (by removing the
ability for Māori to exercise autonomy). Consideration is required regarding mandates,
the
vaccine targets, and COVID-19 vaccine certificates, and the impacts these will have on
different populations.
A rights analysis is outlined in Table 1, below.
under
Released
1982
Act
Information
Official
the
under
Released
Document 6
Section B: Data, evidence, and
stakeholder views
Evidence of proposal impacts
The impacts of immunisation against COVID-19 in 5–11-year-olds are numerous, both direct
and indirect, and have effects not only children but also their whānau, family and
communities.
1982
Direct impacts for children of COVID-19
Health
Act
COVID-19 disease is only rarely severe or fatal in children aged between 5 and 11 years who
will commonly have no, or only mild, respiratory symptoms. However, COVID-19 is still a
significant public health issue in this age group. The risk to this age group is not negligible
and include several health outcomes of concern.
• Throughout the 2021 Delta outbreak there have been over 2200 cases under 12 years
Information
of age (unable to be vaccinated) with 36 hospitalisations. Children aged 5 to 11 have
made up 14.9% of cases in the current Delta outbreak.
• Over the full course of COVID-19 in New Zealand, Māori have been significantly over-
represented in cases (36%), hospitalisations (38%) and deaths (30%). Pacific peoples
Official
have also been over-represented in cases (29%), hospitalisations (36%) and deaths
(24%). In the current Delta outbreak, Māori have made up 52% of cases in 5-11-year-
the
olds, and Pacific children have made up 30% of cases among 5-11-year-olds.
• Childhood immunisation rates have dropped in New Zealand during the COVID-19
pandemic, especially among Pacific peoples and Māori. If diseases such as Measles
under
re-enter New Zealand, this could have significant impacts. The risk of such
preventable disease outbreaks is increased with New Zealand’s borders becoming
more relaxed in early 2022.
• Children with pre-existing health conditions or comorbidities, low socioeconomic
status, or of ethnic minority status (including tamariki Māori and Pacific children) are
Released
at greater risk of severe disease, hospitalisation and ICU admission. Comorbidities in
children with the highest relative risk include:
o asthma
o obesity
o chronic respiratory disease
o neurological or neuromuscular disorders
Document 6
o immune disorders
o metabolic disease.
• Tamariki Māori are over-represented in each of these disease risks.
• Incidence of the severe post-infection Multi-system Inflammatory Syndrome in
Children (MIS-C) is highest in the 5 to 11 age group. MIS-C has occurred more
frequently in children from ethnic minorities in the United States.
• Children can have long-persisting symptoms once acute infection with COVID-19 has
cleared (Long-COVID). Symptoms can be debilitating and distressing for people with
Long-COVID. Even if rates among children is low, if transmission becomes
widespread then the impact of persisting symptoms would be considerable.
1982
• Engagement in non-urgent health services has also dropped (likely in most deprived,
and minority populations, risking increasing health inequities).2
Act
• Globally mortality from COVID-19 among children is low, ranging from 1/10,000
cases in high-income countries to 20/10.000 in low-medium income countries and
100/10,000 cases among infants in low-medium income countries. In the current NZ
outbreak, the majority of cases have been in unvaccinated (64%) or partially
vaccinated (20%) people. Similarly, most of those hospitalised have been
unvaccinated (72%) or partially vaccinated (21%).
Information
• Children and young people are over-represented in cases (37% under 20 years
including 20% under 10 years). At the time, most of these children and young people
would have been ineligible or newly eligible for vaccination., Currently, those aged
Official
under 12 years (15% of NZ’s population) remain ineligible. While children and young
people most often have mild if any symptoms of COVID-19, 10% of New Zealand’s
the
hospitalised cases have been in those under 20 years.
• Over 20% of all cases and more than 7% hospitalisations have been in under-12s.
Social and emotional
under
The COVID-19 pandemic has had significant impacts on how children socialise with families
and communities, with flow on effects to how they handle the emotions of this irregular
period:
• For many the impacts have been neutral, for some even positive as families have
spent increased
Released quality time together in lockdowns.3
2 Blake, D., et al (2022) Accessing primary healthcare during COVID-19: health messaging during
lockdown, Kōtuitui: New Zealand Journal of Social Sciences Online, 17:1, 101-
115, DOI: 10.1080/1177083X.2021.1950780
3 Life in Lockdown: Children and young people’s views on the nationwide COVID-19 level 3 and 4
lockdown between March and May 2020. https://www.occ.org.nz/assets/Uploads/LifeinLockdown-
OCC-Nov2020.pdf
Document 6
• However, many children have suffered increased anxiety and social, cultural and
family relationship stressors, especially those living in poverty prior to the pandemic
or with family violence, addiction and other adverse social contexts.
• A small minority have lost whānau members who have died from COVID-19. Others
have been unable to visit sick and dying whānau members or attend tangi with
gathering restrictions.
• Many children have had to isolate and/or been separated from immediate family
members when whanau have contracted COVID-19, interrupting family and social
relationships.
• Social relationships outside the family with other children have been impacted during
1982
lockdowns and school closures. This is particularly challenging for disabled children
and those without reliable or stable internet access or access to a device.International
Act
border restrictions have separated some children from their families which has had
created stress.
• 6% of children reported worsening relationships with their families4. Large
proportions reported not having anyone in their bubble to talk to about feelings, and
not being listened to.5
Cultural
Information
Children experience a range of cultural impacts during the pandemic, due to both lockdowns
and general COVID-19 restrictions. These include:
• Limits on gatherings and gathering sizes, including at church, tangi, social and
Official
cultural groups.
•
the
Changes to tikanga and other cultural practices to reduce risk of transmission of the
virus.
• Generally speaking, whānau, hapū and iwi systems have responded well to measures
aimed at reducing transmission and risk of COVID-19, through quick mobilisation to
under
identify at-risk whānau and unmet need. Iwi and hapū have often taken a more
cautious approach than that set by health authorities, for example, through choosing
not to re-open marae for events if the community feel the risk is still too high (even if
permitted to under the alert level setting).
Released
4 Life in Lockdown: Children and young people’s views on the nationwide COVID-19 level 3 and 4
lockdown between March and May 2020. https://www.occ.org.nz/assets/Uploads/LifeinLockdown-
OCC-Nov2020.pdf
5 Meissel K, Bergquist M, Kumarich J, et al. The Growing Up in New Zealand COVID-19 Wellbeing
Survey: Part 2: Education. Auckland: Growing Up in New Zealand, 2021.
Document 6
Economic
Children have been affected by the economic impacts of the COVID-19 pandemic. These
include:
• Economic impacts of COVID hit most disadvantaged more substantively, widening
existing inequities for the most deprived, Māori, Pacific, insecurely employed etc.
• Growing Up in New Zealand (GUiNZ) COVID-19 wellbeing survey highlighted
anxieties around household income as a common theme among participant
responses6.
Educational
1982
Children demonstrate abilities to adjust to changes in everyday life due to lockdowns and
pandemic restrictions. However there are impacts on education including: Act
• 75% children report lower satisfaction with education during lockdown, including
anxieties around falling behind due to remote learning periods.
• Deprivation impacted access to education due to inequitable access to necessary
technologies in the learning from home era (the digital divide) 7. Use of apps
increased throughout digital learning, including a high use of apps with age 13+
restrictions.
Information
Direct impacts for children who are immunised
There are a range of likely outcomes for children from receiving the COVID-19 vaccine. Some
Official
are adverse but not serious, and some are clear benefits.
• Non-serious, short-term adverse side-effects of the vaccine, generally comparable to
the
those in adolescents and adults. 8,9
• Protection from serious COVID-19
under
• Reduced risk of hospitalisation/long-term sequelae especially for children with
specific comorbidities or high-risk contexts (e.g., housing).
6 Walker N, Dubey N, Bergquist M, et al. The GUiNZ COVID-19 Wellbeing Survey: Part 1: Health and
Wellbeing. Auckland: Growing up in New Zealand, 2021
Released
7 Life in Lockdown: Children and young people’s views on the nationwide COVID-19 level 3 and 4
lockdown between March and May 2020. https://www.occ.org.nz/assets/Uploads/LifeinLockdown-
OCC-Nov2020.pdf
8 Alamer, E., et al. (2021). "Side Effects of COVID-19 Pfizer-BioNTech mRNA Vaccine in Children Aged
12-18 Years in Saudi Arabia." Vaccines 9(11) DOI: https://dx.doi.org/10.3390/vaccines9111297
9 https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-
positive-topline-results
Document 6
• Protection from long-term consequences of COVID-19, such as Long-COVID
• Reduced time spent isolating at home, greater school attendance, learning,
socialising and relationship development.
• Potentially greater connection with vulnerable whānau and family members where
socialisation or access might otherwise be restricted (eg, in rest home care).
• Potentially greater health service connection and benefits from uptake of wider
healthcare, including greater school attendance and learning.
• Rates of certain rare adverse events among other age groups (eg, myocarditis) have
only become apparent following widespread roll-out. These are not expected to be
higher for the 5 to 11 years age group, and the risk is considerably lower than risks of
1982
the same events from COVID-19. Further data on potential rare side effects will
progressively become available as roll-out continues among children globally.
Act
Indirect impacts for all children of some children being
immunised
• Lower likelihood of severe COVID-19 and hospitalisation among children at higher
Information
risk (eg, disabled children or children with health conditions)
• Probable reduced restrictions on education and recreational activity settings (eg,
school or sports facility closures) Official
• Reduced need and flow-on impacts of other protections that can interfere with
activities and peer relationships, eg, social distancing, isolation and face-coverings.
the
• Potential exposure to adverse social impacts, such as discrimination, blame or
victimisation on the basis of immunisation status and/or conflict such as with protests
in places where children gather
under
• if children are required to use a COVID-19 Vaccine Passport (CVC) there are
implications around access to devices or hard copies, and implications around
interacting with unknown adults. This is a significant matter for children with anxiety
or socially implicated mental health issues.
• Potential reduction in transmission among children due to reduced exposure to
Released
COVID-19, although evidence is limited.10
10 Ainslie, K., et al. (2021). The impact of vaccinating adolescents and children on COVID-19 disease
outcomes, medRxiv.
Document 6
• Opportunities for engagement on crucial ‘catch-up’ immunisations from the national
childhood immunisation programme.
Indirect impacts for whānau and communities of children
being immunised
• Lower likelihood of COVID-19 among people at higher risk (eg, with underlying
health conditions or disabilities) who are in contact with children (especially in
households)
• Greater social connections with children for those at higher risk (e.g., whānau with
underlying health conditions or disabilities), with potentially reduced risk of 1982
transmission (evidence is limited11).
•
Act
Avoiding lost productivity through supervision of unwell/isolating children (women
generally, especially sole mothers and wahine Māori who bear vast majority of
burdens when children unwell)
• Opportunities to engage with other groups (older than 5-11-year-olds) in
immunisation programme, to improve vaccination rates
• Higher immunisation uptake in communities with a high child population, through
Information
family-, whanau- and community-based engagement processes.
• Potentially greater health service connection for whānau of children and benefits
from uptake of wider healthcare Official
• Potential risk of exposure to protests and associated immunisation programme
interruptions when school sites are used as part of vaccination programmes;
the
distraction to learning, and risk of anxiety in children.
Significant impacts on children and young people
under
COVID-19 immunisation has considerable positive impacts for children overall. The vaccine
has a very good safety profile (though data is not yet available on large population cohorts
in the 5 to 11 years age group). Immunisation of children will add to overall population
protection which has been limiting the spread of COVID-19 and allowing a greater level of
social, cultural, educational and economic freedoms for whānau and children.
Released
Children’s wellbeing is enhanced by COVID-19 immunisation as long as access and
availability of opportunities remains open to all children. Any restriction on children’s access
and activities, such as to education or public places, impacts negatively on development. No
such restrictions are justified based solely on whether or not children are immunised.
The positive impacts of immunisation are particularly strong for children in communities
with:
• higher COVID-19 exposure, risks and impacts
Document 6
• higher child populations, particularly where there are high numbers of younger
children ineligible for immunisation
• children at significant risk such as disabled children and children with health
conditions.
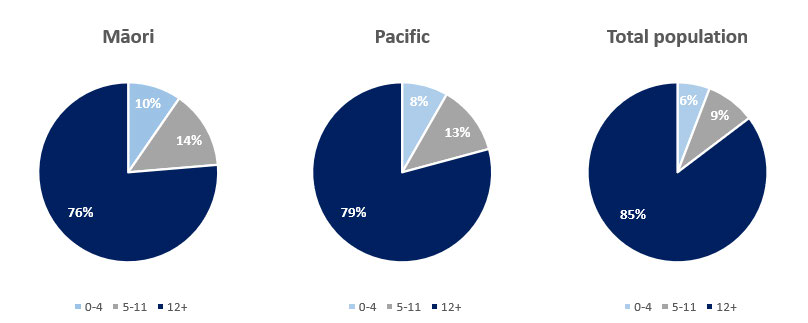
Māori and Pacific communities have young population profiles as shown in figure 1.
Figure 1: Children as part of the population: age structures for Māori, Pacific
and the total New Zealand population
1982
Act
Information
Official
Impacts on different groups of children and young people
the
Māori
There are an estimated 115,562 tamariki Māori aged 5 to 11 years (14% of the Māori
population and 24% of the NZ population of 5-11-year-olds). In the 2021 Delta outbreak,
under
tamariki Māori have made up over half of infections under 20-years of age, suggesting
disproportionate risk of infection and severe COVID-19 impacts. These impacts may be from
higher exposure associated with inter-generational living, housing instability, household
crowding and in-person connected communities, from higher rates of respiratory and other
long-term health conditions such as rheumatic heart disease, disabilities, and from poor
standards of care or discrimination within health systems. For similar reasons, tamariki Māori
Released
may have potential risk from at-home self-isolation measures.
Māori are highly represented in areas with both active transmission of COVID-19 and with
lowest vaccination rates. The impacts of vaccination on tamariki Māori include reduced
overall risk of severe disease, opportunities to reach whānau members who are yet to be
vaccinated or receive second doses, through whānau-based implementation approaches.
Document 6
Pacific
There are an estimated 49,398 Pacific people aged 5 to 11 years (roughly 17.5% of the Pacific
population and 10.5% of NZ population aged 5 to 11 years). The majority of Pacific peoples
reside in the Auckland region and 29% of cases and 37% of hospitalisations in the 2021 Delta
outbreak have been in Pacific peoples. This suggests a disproportionate risk of infection and
severe COVID-19 impacts for this group.
These impacts may be from higher exposure associated with inter-generational living,
household crowding, in-person connected communities, higher pre-existing condition
burden (including rates of respiratory and other long-term health conditions such as
rheumatic heart disease), and disabilities. For similar reasons, Pacific children may have
potential risk from at-home self-isolation measures. Over 25% of Pacific children are
1982
experiencing material hardship (highest of any ethnic group) and disproportionate rates of
obesity, and preventable and chronic illnesses which increase risk of severe illness from
Act
COVID-19.
Pacific peoples are overrepresented in areas with active transmission, and vaccination rates
in this population lagged that of more advantaged populations. Full immunisation rates for
Pacific children at 2 years of age has dropped to 67.4 percent in July 2021 compared with
93.8 percent in December 2019. The impact of vaccination among Pacific children includes
overall reduced risk of severe disease and subsequent hospitalisations, positive impacts on
Information
school attendance and educational attainment and opportunities to engage on childhood
vaccine progress, and to reach family and community members who are yet to be vaccinated
or receive second doses through community-based approaches. The overall youthful
distribution of the pacific population of New Zealand also means vaccination of this group
Official
contributes to greater overall vaccination rates for Pacific peoples.
Evidence suggests significant hesitancy to return Pacific children to school even outside
the
school closure periods. Immunisation is likely to reduce this hesitancy and improve
educational outcomes for Pacific children.
Similar risks and impacts would also apply to Pacific countries outside of Aotearoa
under
New Zealand, such as in Cook Islands, Niue and Tokelau, which have proportionately high
child populations.
Disabled children
As at the 2013 census, there are roughly 50,000 children between the ages of 5 and 11 with
Released
identified disabilities. Disabled people are at high risk of severe disease from COVID-19
infection. This risk is multifactorial, through increased risk from infection itself, reduced
access to routine healthcare, and the adverse social impact of pandemic mitigation11.
Disabled children are more likely to live in poverty and in conditions which make respiratory
11 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00625-5/fulltext
Document 6
illness more severe. Furthermore, Māori and Pacific children have higher than average
disability rates, increasing their already increased overall risk from COVID-19.
The potential impact of vaccinating disabled children included reducing their overall risk
from COVID-19 and opportunities to engage with whānau, family, caregivers and children
themselves on opportunities to vaccinate whānau/caregivers, broader health and wellbeing,
pandemic impacts (education, social services etc) and the possibility for engagement with
available support services/packages. There is growing evidence of parental hesitancy to
vaccinate children with neurodevelopmental disabilities (some of the highest-risk children)
against COVID-19. Tailored communications will be required to confer the proposed benefits
to this group.12,13
Long-term illness
1982
A number of chronic conditions increase the risk of infection with COVID-19. The WHO
Act
identify older age, obesity, type 2 diabetes, asthma, heart/pulmonary disease, neurological,
neurodevelopmental and neuromuscular14 conditions. Maori are over-represented in many
of these disease risks. Paediatric cancer patients are at increased risk due to
immunocompromising disease and treatments, as well as delays in treatments.15It is difficult
to estimate how many children in New Zealand have any type of chronic condition, and the
amount of intersectionality in these populations. Examples, however, include 11.9% of
children under 14 with Asthma, 30.8% of children under 14 who are obese or overweight –
Information
both of which disproportionately impact Māori and Pacific children. Furthermore, diseases of
poverty such as bronchiectasis, rheumatic fever and rheumatic heart disease are all
vulnerabilities for severe COVID-19 and almost exclusively impact Māori and Pacific.
The potential impacts of vaccinating children with chroni
Official c conditions include reduced risk
from infection and severe illness from COVID-19, and, as with disabled children, provides
opportunities to engage with children and families on COVID-19 vaccine status, disease-
the
management throughout the pandemic, and eligibility for support.
under
12 Aggarwal, S., et al. (2021). "Vaccine Hesitancy Among Parents of Children With Neurodevelopmental
Disabilities: A Possible Threat to COVID-19 Vaccine Coverage." Journal of child neurology:
8830738211042133 DOI: https://dx.doi.org/10.1177/08830738211042133
Released
13 Choi, K., et al. (2021). "Parent intentions to vaccinate children with autism spectrum disorder
against COVID-19." Journal of pediatric nursing DOI: https://dx.doi.org/10.1016/j.pedn.2021.11.019
14 Aiano, F., et al. (2021). "COVID-19 vaccine given to children with comorbidities in England,
December 2020-June 2021." Archives of disease in childhood DOI:
https://dx.doi.org/10.1136/archdischild-2021-323162
15 https://onlinelibrary.wiley.com/doi/full/10.1002/pbc.29397
Document 6
Children in the care of Oranga Tamariki
Approximately 2000-2500 children between 5 to 11 years of age are in the care of Oranga
Tamariki. Children in care are predominantly Māori, Māori and Pacific, or Pacific peoples
(68% have Māori as one of their recorded ethnicities). They are more likely to be disabled,
and to have high and complex needs than the general population (including higher rates of
mental health needs and of Fetal Alcohol Spectrum Disorder).
When children first enter care, there is a higher likelihood that they will be in placed multiple
homes in a relatively short period of time and are often with multiple other children while
more stable, enduring care is established. Family Group Homes pose a particular risk as the
placements are often at short notice and in environments where there may be up to six
children at a time.
1982
Children entering care for the first time are less likely to be fully immunised when they come
Act
into care than the general population, indicating that they are less engaged with primary
care. This means flexible and tailored ways of reaching children on the cusp of care and their
caregivers/whānau are needed to ensure high vaccine uptake
For immunisation of children in care, Oranga Tamariki currently requires guardianship
consent. Many children in care are in family/whānau care arrangements and only a few
children are in sole guardianship with Oranga Tamariki. This means consent to vaccination is
Information
a complex issue and will require working through at an operational level. Special
consideration needs to be given regarding the chief executive’s responsibilities to children in
the care of Oranga Tamariki.
Most children who contract COVID-19 will isolate at home with their parent/s and whānau.
Official
Children in care would isolate with their caregivers, so the requirement to isolate will have an
additional impact on their ability to maintain their contact with their parent/s and whānau.
the
There have already been significant disruptions to maintaining contact as a result of the
lockdowns.
In summary, children in care are considered among the most vulnerable children in New
under
Zealand. They are at greater risk of contracting COVID-19 and suffering more serious effects
from it, than the general 5-11-year-old population. Achieving high rates of vaccination for
these children provides the greatest chance of minimising these risks and protecting this
group. This must be done in close consultation with whānau and caregivers, in a manner that
upholds mana tamaiti, whakapapa and whanaungatanga.
Released
The potential impact of vaccination of children in care is reduced risk for severe illness
among a population with multiple risk factors.
Children in poverty or deprived communities
Nearly a quarter of New Zealand’s children are growing up in households considered to be
in poverty16, and one in five children are living in benefit-supported households, the majority
16 https://dpmc.govt.nz/sites/default/files/2020-07/child-poverty-related-indicators-2020.pdf
Document 6
of which are sole-parent households17. High deprivation is associated with stress, chronic
illnesses, low health-literacy and irregular and infrequent healthcare access and is a
considerable risk factor for infection and severe-illness from COVID-19. As discussed in
above section, tamariki Māori, Pacific children and disabled children are overrepresented in
deprived communities and have a multitude of COVID-19 risk factors on top of poverty.
The impacts of immunisation for children growing up in deprived communities include an
overall reduced risk of severe illness, opportunities to engage with whānau and families on
vaccine status, and presents additional opportunities to engage and provide wellbeing and
social support to at risk communities.
Children in multiple households
1982
Similarly to children in care, children in shared custody arrangements are at an increased risk
of exposure to COVID-19 due to the transitional nature of their custody (moving between
Act
homes on regular basis), especially during periods of active transmission in their
communities. Furthermore, there is inevitable cross over between this population and other
risk-factors such as deprivation and chronic illness.
The impacts of vaccinating this population include the reduced risk of severe disease, and a
reduced risk of exposure and transmission between households and beyond (e.g., schools
and communities). Further impacts include opportunities to engage with families on
Information
vaccination status, and provide engagement with other wellbeing and social services.
Implications for Tamariki Māori
To date, vaccination of Māori has been slower than for non-Māori, particularly for younger
Official
age groups. Furthermore, tamariki Māori represent roughly 27% of the 5-11-year-old
population, and have made up over half of cases under 20 years of age in the current
the
outbreak, likely due to their multifactorial risk profile. Their inclusion in the vaccine eligible
population would represent a significant proportion of the Māori population yet to be
vaccinated, and an equally significant proportion of the 5–11-year-old population for any
under
paediatric COVID-19 vaccine immunisation programme to focus on reaching.
Te Tiriti o Waitangi obligations, including oritetanga (equity), tino rangatiratanga, options,
active protection and partnership, continue to be essential in the planning of immunisation
programme rollout, and lessons from the programme so far will be utilised in leveraging
existing partnerships, including the COVID-19 response Iwi chairs forum.
Released
While the Ministry plans to use existing infrastructure such as DHBs, Primary Care and
Community centres as the primary delivery mechanisms, a multi-pronged approach will be
undertaken to co-design this service with our hauora providers to meet the needs of tamariki
and their whānau. In addition to receiving guidance and advice from our Māori experts on
the IIAG, CV-TAG, and the Disability Advisory Group of Tātou Whaikaha, the Ministry (CVIP
17 https://www.msd.govt.nz/about-msd-and-our-work/publications-
resources/statistics/benefit/index.html
Document 6
Equity team and Māori Health Directorate) will engage with the existing Māori health
providers to understand what additional supports and resources may be required to
implement this service successfully to tamariki, including relevant Health Service User and
CVIP engagement data required to target their efforts efficiently.
The implications of these proposals include cooperation on achieving equitable outcomes
for Tamariki Māori, opportunities to engage with whanau and communities on vaccination,
and the protection of tamariki as taonga and future kaiarataki (leaders) of hapu and Iwi.
National Distribution of 5 to 11 Age Group
Figure 2 illustrates the distribution of 5 to 11 years olds throughout New Zealand based on
1982
Health Service User data, with additional breakdown demonstrating the proportion of
Tamariki Māori and Pacific children in each DHB region. Population distribution data will
inform immunisation programme efforts for focus resources on reach high-risk popul
Act ations.
Information
Official
the
under
Released
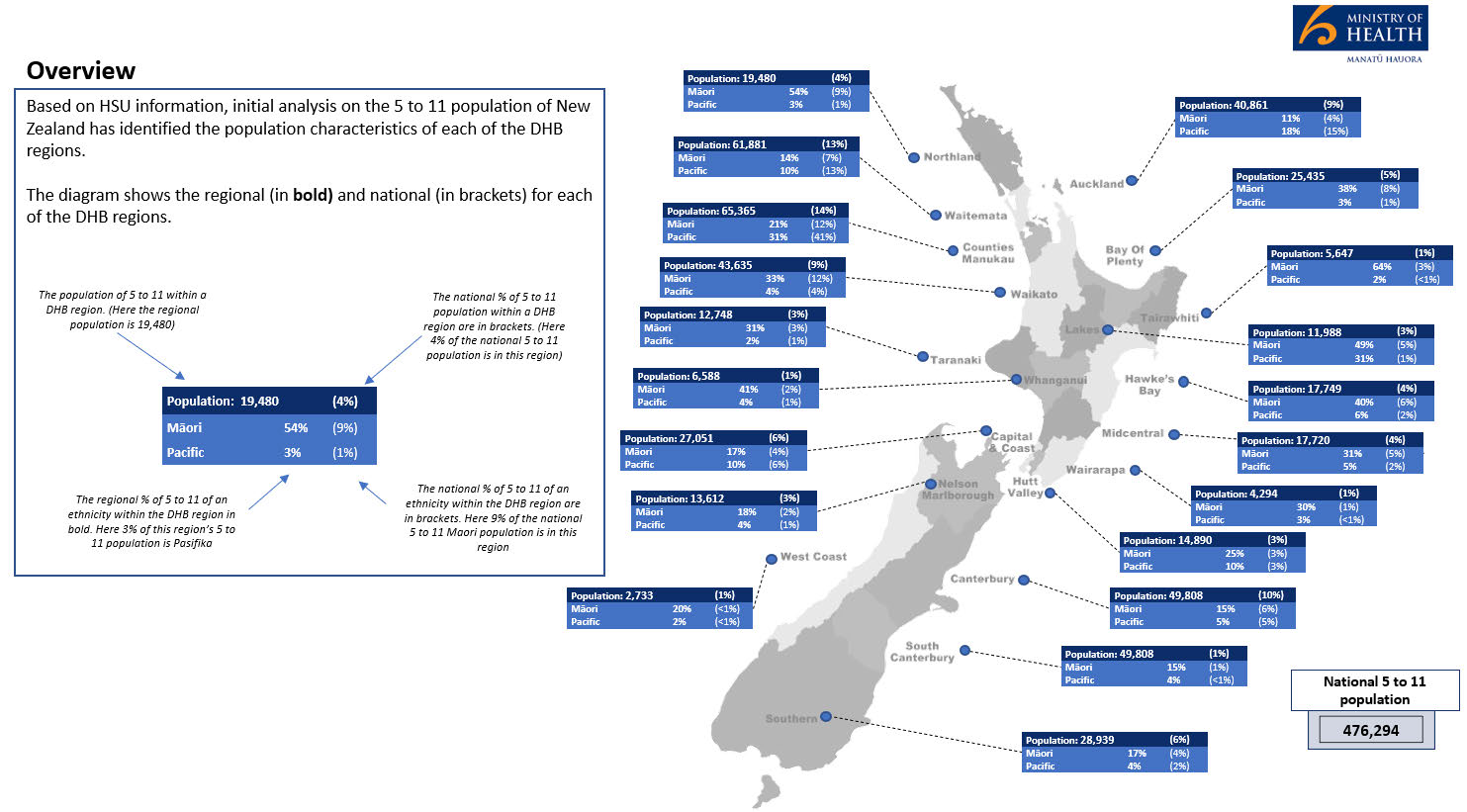
Document 6
Figure 2: Distribution of 5 to 11 year olds throughout New Zealand
1982
Act
Information
Official
the
under
Released
Document 6
Views of Children
Consultation with stakeholders with sources and experience on the views of children with
respect to the pandemic and vaccination included a number of relevant themes.
• Enriched connection with family/whānau and friends through mutual support, and
engagement on digital learning 18
• Exercising manaaki, connecting to culture and community in innovative and
supportive ways
• Financially secure ‘bubbles’ – such as concerns about household income throughout
the pandemic, and awareness and anxieties of constraints 19
1982
• Flexibility and choice about the use of their time during lockdown and digital learning
periods 20
Act
• Enjoying quiet, safe environments during lockdowns
• Making sense of the situation, integrating it into their life story
• Positive experiences through times of risk 21
• Supporting decision making for guardians of children aged 5 to 11 years by
Information
providing consumable and culturally relevant information about the vaccine, and how
to discuss immunisation with children
• Children’s ability to seek out their own information, subsequent exposure to
misinformation, and providing accurate information in formats that children can
Official
digest
the
The proposed 5 to 11 years immunisation programme and the range of direct and indirect
impacts would support a number themes present in the various reporting on children’s
views.
under
18 Life in Lockdown: Children and young people’s views on the nationwide COVID-19 level 3 and 4
lockdown between March and May 2020. https://www.occ.org.nz/assets/Uploads/LifeinLockdown-
OCC-Nov2020.pdf
Released
19 A snapshot of Life in Lockdown: Children’s Health, Wellbeing, and Education. Growing Up in New
Zealand (GUiNZ)
https://www.growingup.co.nz/sites/growingup.co.nz/files/documents/Wellbeing_Survey_Snapshot2-
4b%20FINAL.pdf
20 Life in Lockdown: Children and young people’s views on the nationwide COVID-19 level 3 and 4
lockdown between March and May 2020. https://www.occ.org.nz/assets/Uploads/LifeinLockdown-
OCC-Nov2020.pdf
21 Life in Lockdown: Children and young people’s views on the nationwide COVID-19 level 3 and 4
lockdown between March and May 2020. https://www.occ.org.nz/assets/Uploads/LifeinLockdown-
OCC-Nov2020.pdf
Document 6
Consent to vaccination
The United Nations (UN) have asked governments to prioritise children’s rights in the
development of policy related to COVID-19 in a manner that is consistent with the UN
Convention on the Rights of a Child. Article 5 of the Convention stipulates respect for the
responsibilities, rights and duties of parents and guardians in a manner consistent with the
evolving capacities of children.
While there is no lower limit to the age at which individuals can provide consent to
vaccination, we anticipate children aged 5 to 11 years will be accompanied by parents or
whānau members.
Other stakeholder views
1982
Stakeholders have emphasised the importance of culturally acceptable communication and
Act
engagement throughout the implementation design and delivery so that all children have
equal opportunities to be immunised.
Culturally appropriate and safe communication for tamariki Māori, whānau, hapū and iwi is
essential in creating an equitable immunisation programme, communicating options, and
informing decision making and tino rangatiratanga. Whānau-based approaches are essential
and should be emphasised, including clear messaging that all whānau are welcome in the
Information
process, welcome to ask questions, and invited to participate in getting their vaccine.
Messaging in te reo Māori is also essential.
Information for Pacific Aiga should include information tailored for Pacific children,
emphasise the protection of children in its messaging, and focus on mothers as the primary
Official
decision makers regarding the health of children. Communications for disabled people
should focus not only on materials for disabled children but also consider children living in
the
disabled households and the needs of these family and whānau to understand the process,
and the systems in place to support their participation in the immunisation programme.
Growing evidence suggests that vaccine hesitancy is highest among school-aged children
under
and parents in socioeconomically deprived communities and populations, who consume
more social media, and have feelings of isolation and marginalisation. These populations are
already experiencing disadvantage and poor vaccine rates. 22 23 Efforts should be made to
Released
22 Fazel, M., et al. (2021). "Willingness of children and adolescents to have a COVID-19 vaccination:
Results of a large whole schools survey in England." EClinicalMedicine 40: 101144 DOI:
https://dx.doi.org/10.1016/j.eclinm.2021.101144
23 McKinnon, B., et al. (2021). "Social inequalities in COVID-19 vaccine acceptance and uptake for
children and adolescents in Montreal, Canada." Vaccine 39(49): 7140-7145 DOI:
https://dx.doi.org/10.1016/j.vaccine.2021.10.077
Document 6
tailor and target communications for these populations in order to maximise effectiveness
and reach of immunisation.
Guidance on promoting child wellbeing during the pandemic
A number of stakeholders have raised the need for guidance on how to best provide for
children’s access and enjoyment of developmental, recreational, social, cultural and other
activities and public places during the pandemic. This guidance is needed by a wide range
of government, non-government and business operators, and applies to children individually
and in groups.
The guidance will need to cover access for children in mixed age groups, where older
children may have vaccine certificates and younger children not. It will be needed early after
1982
immunisation starts for this age group, especially by schools as they start planning for the
2022 school year.
Act
Ongoing engagement through development and implementation
Stakeholders have informed the development of this Child Wellbeing Impact Assessment
and will continue to inform the decision to use a paediatric vaccine product, the
implementation approach and implementation plans at a District Health Board Level.
The high-level engagement plan for immunisation consideration and implementation is
Information
outlined in the table below.
Official
the
under
Released
Document 6
High level engagement plan
Stage of
Description and
Lead
Engagement
process
purpose
Purpose
Level
Who –
Who – external
Timeline
internal
Child impact
Formal assessment of MoH
Share
Involve
CVIP, CHSR –
Office of Children’s
Draft 10
assessment
child wellbeing
SSP –
information
STA
Commissioner,
Dec 2021
impacts, completed in System
Improve
Māori Health
Ministry of
Conducted in
order to inform a
Enablers proposals
PHP – Pacific,
Education,
Final 20
tandem with
subsequent decision
Understand
FCH, Imms
Oranga Tamariki,
Dec 2021
regulatory
on whether and how
reactions
HSSI – H&D
Growing Up in NZ,
assessment and
to use vaccines for
Generate
intelligence
Social Wellbeing
science and
children aged 5-11
support
Disability, MHA Agency
technical advice
years
Consult
IIAG
Te Puni Kōkiri,
1982
CV-TAG
Ministries for Pacific
Tātou
Peoples, Women,
Whaikaha
Ethnic Communities,
Act
Disability
Office for Disability
Advisory Group Issues,
Treasury,
DPMC
Decision to use Advice to Cabinet
MoH
Improve
Involve
CVIP
Ministers with
SSP –
proposals
Draft 20
Pre-requisites
recommendations on System
Generate
Consult
CHSR – STA
Office of Children’s
Dec 2021
include Medsafe
whether and how to
Enablers support
Māori Health
Commissioner
approval for use
use vaccines for
PHP – Pacific
Ministry of
Final 22
and supplier
children 5-11 years,
Education,
Dec 2021
agreement. Inputs submitted after
Oranga Tamariki,
Information
include CV-TAG
Medsafe has granted
Te Puni Kōkiri,
and IIAG advice
approval for the
Ministry for Pacific
vaccine to be used in
Peoples,
New Zealand
MFAT,
Treasury, DPMC
Implementation Service design
MoH
Identify
Collaborate IMAC
DHBs,
Official
approach
approach for
CVIP
problems /
Involve
IIAG
Oranga Tamariki,
10 Jan 22
immunisation of
opportunities Consult
Tātou
Ministry of
children, including
Improve
Whaikaha
Education,
Plus
workforce,
proposals
Disability
Primary/community ongoing
the
technology, delivery
Build
Advisory Group health
through
models, distribution,
relationships
Q1 22
prioritisation
District
Detailed plans for
DHBs
Problem solve Empower
Māori, Pacific,
Iwi, hapū, local
Evolving
implementation delivery models for
Improve
Collaborate disability leads communities, health
under
ongoing
plans
the range of
proposals
Involve
Paediatricians, and disability
through
communities in the
Build
Consult
PHO clinical
communities,
Q1 2022
district, including
relationships
leads
groups, gangs,
providers, facilities,
Hauora, primary
communication,
care, other health
promotion, tailoring
providers,
to local needs and
Schools, kōhanga,
preferences
child service
providers, Crown
Released
agency regional and
local branches,
Health and social
service providers,
NGOs
Document 6
WHO guidance
The World Health Organization (WHO) issued an Interim statement on COVID-19 vaccination
for children and adolescents (updated 29 November 2021)24. It states that:
• Countries should consider the individual and population benefits of immunising
children in their specific epidemiological and social context
• Benefits go beyond direct health benefits – minimising disruptions to education and
maintenance of overall well-being, health and safety are important
• Attaining high coverage of high-risk groups such as older people, those with chronic
health conditions and health workers, including booster doses, should be prioritised
before children and adolescents
1982
• Global sharing through the COVAX facility should be prioritised before vaccination of
Act
children and adolescents who are at low risk for severe disease.
This child wellbeing impact assessment considers the individual and population benefits of
immunising children in the specific epidemiological and social context of New Zealand and
of population groups within New Zealand. It considers benefits beyond direct health
benefits, including minimising disruptions to education and maintenance of overall
wellbeing, health and safety.
Information
The findings of this assessment support immunisation of the wider population as the most
important protection for the group of children 5 to 11 years.
This assessment sits alongside New Zealand’s plan to offer COVID-19 paediatric vaccine to
the countries of Polynesia (the Cook Islands, Niue, Samoa, To
Official kelau, Tonga, and Tuvalu) to
support their child immunisation plans. Most of these countries have high child populations
and have indicated their strong interest in
the providing immunisation for their children.
It also sits alongside New Zealand’s commitment to global equitable access to COVID-19
vaccines, including a contribution of over 2 million vaccine doses to the COVAX Advance
Market Commitment to support vaccination of adult populations in developing countries
under
worldwide.
Released
24 https://www.who.int/news/item/24-11-2021-interim-statement-on-covid-19-vaccination-for-
children-and-adolescents
Document 6
Section C: Summary of Impacts
Conclusion of impacts on policy proposal
COVID-19 has wide ranging impacts on children and young people across a variety of
domains and presents a significant public health issue for children aged 5 to 11. The impacts
of immunisation against COVID-19 for children are equally wide ranging and include:
• reduced risk of severe disease and hospitalisation, especially for high-risk populations
including tamariki Māori, Pacific children, disabled children and children with health
1982
conditions, children living in poverty and children in the care of Oranga Tamariki
• protection from serious outcomes such as Multi-system Inflammatory Syndrome in
Act
Children (MIS-C) and Long-COVID
• educational stability and satisfaction
• opportunities to re-engage in the national childhood immunisation programme
• opportunities to engage with family and whānau on health and social support
requirements.
Information
COVID-19 does not impact all children equitably. Tamariki Māori, Pacific children, disabled
children and long-term illness, and children in care are all at higher risk of severe disease,
hospitalisation, and have a range of indirect impacts on their lives and development due to
Official
the pandemic. Immunisation therefore has differing impacts on each of these groups,
reducing the inequitable risk they bear, and providing opportunities to engage them in
various health and social services which c
the an reduce the overall impact of the pandemic on
them and their families and whānau.
Tamariki Māori bear a significant burden of the pandemic, including high rates of cases and
hospitalisation. Focus is required in
under order to uphold the Crown’s Te Tiriti obligations of
equity, active-protection, partnership, options and tino rangatiratanga. A multi-pronged
approach which includes engagement with iwi, hapū and community stakeholders and Māori
health providers will enable cooperation on achieving equity and the protection of tamariki
Māori as taonga.
Prioritising the rights of children is crucial when considering immunising this cohort. Analysis
Released
of this proposal against the Convention on the Rights of the Child indicates that
immunisation of 5 to11-year-olds should enhance the rights of children. However, including
5 to 11 year olds in vaccine mandates, requirements for COVID-19 vaccine certificates, or
vaccine targets would risk children’s ability to engage in activities crucial to their
development.
Document 6
The benefits to children of COVID-19 immunisation, while considerable, do not outweigh the
benefits to their development of full access and participation in education, development,
recreation and community activities and public places.
A wide range of stakeholder views have informed this impact analysis. These include:
• Office of the Children’s Commissioner
• Ministry of Education
• Ministry of Social Development
• Oranga Tamariki
•
1982
Te Puni Kōkiri
• Ministry for Women
Act
• Ministry for Ethnic Communities
• Ministry for Pacific Peoples
• Department of the Prime Minister and Cabinet
• Office for Disability Issues
Information
Recommendations
Offering COVID-19 immunisation to children 5 to 11 years
Based on this impact analysis, it is recommended that:
Official
• immunisation of the wider population continues – it is important to protect children
the
and promote their wellbeing
• immunisation of children should proceed and be offered to all aged 5 to 11 years – it
adds protection and promotes children’s development with or without high levels of
under
population immunisation
• immunisation of tamariki Māori requires high and timely focus – Māori have suffered
high pandemic impacts, remain at high risk and have a high child population with
10% of Maori under 5 years old and ineligible for vaccine
• immunisation of children should be encouraged, but not subject to restrictions under
Released
the Protection Framework or any other restrictions based on vaccination status
• immunisation of children should where possible promote whānau wellbeing, be
offered in multiple ways to suit a wide range of families and groups, and cater
especially for Pacific peoples, disabled children, children with health conditions and
children with family members who are disabled or have health conditions, children
and families living in poverty, and children in the care of Oranga Tamariki.
Document 6
Communication
Achieving equitable outcomes for the various groups explored in this analysis will depend on
tailored and culturally appropriate communication at all levels and in all communities.
It is important that communications are designed in a way to make sure that parents or
other decision makers are well-informed about the risks and benefits of vaccination when
consenting on behalf of children.
Children have the right to appropriate guidance based on their capacities. Communications
should therefore also encourage and guide parents and guardians in discussing
immunisation with their child/children. As recipients of the vaccine, children require specific
communications that help answer their questions such as on whether the vaccine is safe or
1982
what the process will be like; separate information should be developed that it suitable and
user-friendly for this diverse age group.
Act
Maximising opportunities for children’s wellbeing and development
Children should enjoy full access and participation in opportunities and public places. It is
unlikely restrictions that are solely based on whether or not a child is immunised will be
justifiable.
Information
Official
the
under
Released